
If you had a suspicious lesion or lump, would you trust a computer algorithm to spot, diagnose, and recommend a treatment for a possible tumor? While some clinicians, oncologists and radiologists resist doing so, most still agree that using artificial intelligence to aid in the identification, diagnosis, treatment, and prognosis of cancer in their patients represents the wave of the future.
Dr. Bipin Gaikwad, a postdoctoral researcher at the Tufts University Institute of Artificial Intelligence (TIAI), once worked in smart surveillance, a technology that uses AI to develop security systems to prevent terrorist attacks. Now, he has turned his fascination with AI in a very different direction. Recently, while working to complete a postdoc at Tufts University, he contributed to a paper on the use of AI in medicine published by Tufts researcher Dr. Thomas Schnelldorfer. Their work focuses on how to use AI during minimally invasive laparoscopies to determine whether gastrointestinal lesions are benign or malignant.
The connection between counterterrorism surveillance and cancer detection comes down to the power of AI. In these disparate fields, AI finds patterns in images that human eyes miss. According to Dr. Gaikwad, smart surveillance accesses more than one million images for its AI algorithms to learn and train on, compared to biomedical data, which only has thousands to work with. He expects this latter number to greatly increase, allowing AI to come up with more robust decisions supported by larger numbers of images. Then, it will better distinguish between malignant and benign tumors as it more accurately captures small details that radiologists, pathologists, surgeons, or other clinicians can rely on when making life or death decisions.
What Is Artificial Intelligence?
AI is the multidisciplinary branch of computer science that focuses on building smart machines that can accomplish tasks that normally require specialized human expertise and judgement. Sometimes machine learning algorithms can complete tasks better than the best diagnosticians, clinicians, and pathologists.
To build algorithms for cancer screening, programmers feed images of tumors known to be benign or malignant into the computer. This data trains the AI to identify each of these conditions. Programmers do this thousands of times, a process they call training the model. An algorithm’s guess comes from its training on the model. If it comes up with an incorrect probability, its error becomes part of the improved calculation going forward. Over time, the algorithm learns subtler patterns, including color, texture, vascular patterns, things that humans may not consciously perceive. The final trained algorithm is a mathematical function that takes an image and outputs the probability of metastasis.
These models are starting to have real success: In their paper, Schnelldorfer and Gaikwad report that surgeons who did not use AI in evaluating biopsied peritoneal lesions had 52% accuracy, while those who used computer-assisted staging laparoscopy achieved a 66% accuracy rate.
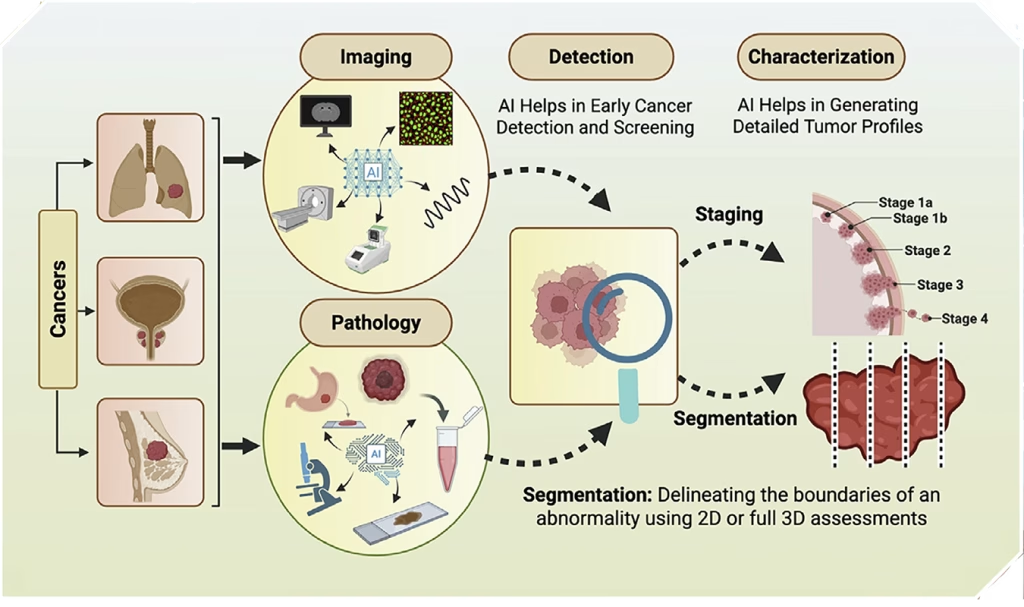
AI comprises several important subfields that help with this clinical work: machine learning (ML), deep learning (DL), and natural language processing (NLP). ML learns from large, structured datasets—such as lab results, genomic profiles, and clinical records—to identify patterns that predict outcomes, classify cancer subtypes, and flag patients at risk. DL, a subset of ML, uses layered neural networks, or architectures, to perform image segmentation, or the division of a tumor’s digital image into discrete regions. DL allows for more-precise tumor boundary definition, staging, and measurement than manual tracing does, because it is less vulnerable to human bias. NLP complements these tools by extracting relevant data from clinical reports and patient records, which AI then integrates with images to provide a more complete picture of tumor biology.
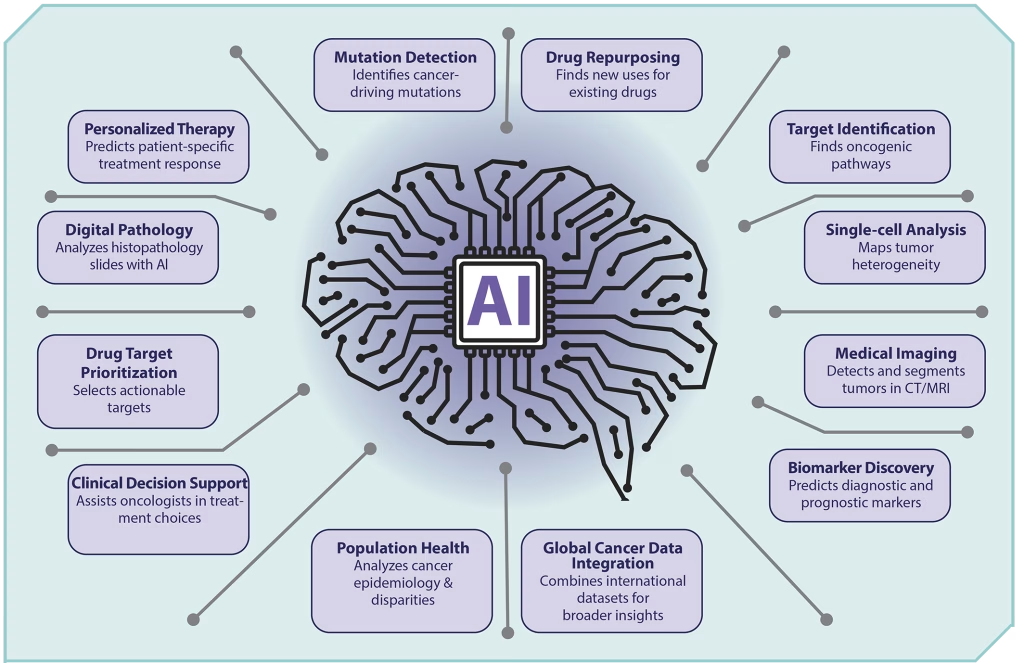
Medical researchers expect these AI tools to help provide earlier and more accurate diagnoses than trained examiners can by just using their eyes because AI can identify minute details that point to underlying patterns and abnormalities. Developers hope to combine various AI tools to expand the sensitivity and accuracy of drug development, the interpretation of complex images, the identification of cancers and cancer biomarkers, the analysis of mutations, the choice of the best therapies, and accurate prognoses of remission or relapse.
Diagnosing Cancer Through the Use of AI
More than 200 distinct cancers, with completely different behaviors and responses to treatment, develop in humans. The cancers with the highest incidence include lung (12.4%), breast (11.6%), colorectal (9.6%), prostate (7.3%), and stomach (4.9%), according to the International Agency for Research on Cancer (IARC). Clinicians use different approaches to diagnose these cancers, including cytology, histology, cytogenetics, and both pathology and radiographic imaging, such as CT-scans or MRIs. AI can aid in diagnosis by integrating the results of all these methods with relevant clinical data, improving clinical accuracy and contributing greatly to patient survival.
Doctors very much need this new approach. Despite recent, revolutionary developments in identifying, diagnosing, and treating cancer—for example, new immunotherapies for melanomas—the IARC predicted 19.9 million new cancers in 2022, along with 9.2 million cancer-related deaths. This prediction was spot on, with 9.7 million deaths in that one year.
Fortunately, many innovations are pushing AI forward in oncology. For example, the international expansion of Electronic Health Records, large volumes of patients’ digitized data in storage and readily accessible to doctors, now advance research in the early diagnosis of cancer. The FDA has used this data to approve an AI software platform that can detect and track pulmonary nodules longitudinally, or through time, to better predict lung malignancy. Researchers have also developed deep neural networks, an advanced ML model inspired by the human brain, which spot enlarged lymph nodes and small colon polyps on CT-scans.
In addition, researchers now use AI algorithms for cancer imaging and detection in a DL system that uses whole slide images of radical prostatectomies (prostate removals) to assess Gleason scores with greater accuracy than pathologists can. In one breast cancer screening study, AI models’ scores matched expert reader performance and sometimes exceeded it by 11.5%.
Integration of OMICS data
Due to the varied and complex nature of tumor biology, researchers rely on AI to understand the tumor landscape and to improve how to target drugs to specific cancers. Their multimodal approach uses data from the following sources:
- transcriptomics (the study of all RNA produced by an organism’s genome)
- radiomics (the use of analytics to obtain hidden data from medical images)
- metabolomics (the study of small-molecule metabolites and products of metabolism) and
- genomics (the study of an organism’s genome).
They then fuse this data with the identification and analysis of cancer biomarkers. These AI-linked “omics” data sources have been useful in clinical model development. For example, a multiomics data study of 23,000 patients with 32 different kinds of cancer resulted in a better understanding of cancer biology.
Radiation Dose
Another AI innovation, deep neural network (DNN), helps doctors calculate radiation dosages for diagnostic evaluation and therapy. To get precise images of tumors, radiation dosage must be correct. With a high tissue background, clinicians must increase the dosage to get a better signal over the interfering background noise. In other words, the image quality and signal-to-noise ratio directly relate to the radiation dose. Without the help of AI, an oncologist may not know how to appropriately reduce the radiation exposure for each exam. DNN can transfer low-dose, lower quality, high noise CT images into higher quality, low noise images, mapping data from one space to another, assisting the radiologist in reducing radiation doses and minimizing normal tissue exposure to radiation.
AI can also detect metastatic cancer cells, including the tiny foci in sentinel LN cells, the first lymph nodes where cancer cells typically spread from a primary tumor. Even with the typical variation in tissue samples, the AI algorithm performs without a hitch.
Biomarker discovery
AI further assists in identifying specific drugs to target different cancers. It helps to generate novel molecular structures that researchers can then develop into drugs. AI speeds the discovery of tumor biomarkers that drugs can target and forecasts patients’ resistance to drug treatment. By mining genomic data, AI can find genetic variants and tiny, difficult-to-detect mutations that link to disease. AI-driven virtual screening speeds up the drug-compound selection process and tailors the number of compounds that require experimental investigation. This faster drug investigation process also makes it simpler to predict how chosen drug molecules will interact with their targets.
Challenges That Impact the Future of AI
In the last seven years, the number of FDA-approved medical imaging AI products for radiology has increased greatly, and we expect this upward trend to continue. For AI tools to be effective in clinical decision-making, however, developers need to effectively explain them to ensure that clinicians understand and trust the AI reasoning as proven and reliable. Tool developers must therefore ensure that they make the computer code that they use readily available.
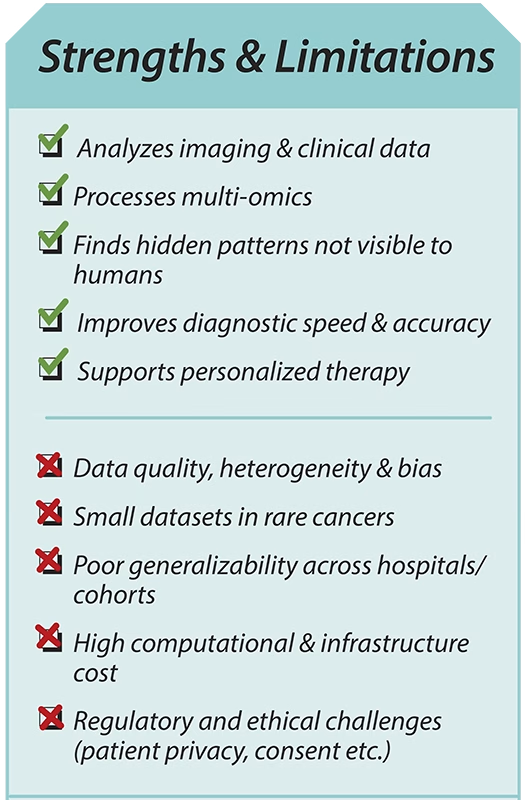
Another limitation for medical AI developers relates to the current lack of many large, publicly accessible, annotated-image datasets, especially for such rare cancers as those affecting soft tissue and bones. In addition, data quality can be variable and heterogeneous, and all combined data must be high quality and unbiased to be included in a computer training set. Lastly and importantly, all data, to be applied and relevant, must reflect real-world usage.
AI Tools Do Come with Risks
Developers will face legal and regulatory issues involved with data privacy and the protection of patients’ records as they work to expand datasets necessary to train AI for medical use. They must keep patients’ data well-locked to keep it safe as they work with it. When they combine previously validated, small, single-institution datasets, they must annotate, revalidate, and retest the resulting larger dataset. Tool developers must also have an idea about possible errors before applying the algorithms to their final large models.
Finally, the ultimate use of these AI tools does come with some enormous risks. In the tragic case of misdiagnosis and possible loss of life, who is legally responsible when AI contributes to the decision-making process? Who takes responsibility for a tragedy? Tool developers? Clinicians? Hospitals? Insurers? We must debate and determine appropriate regulations as AI moves into general clinical usage.
Clearly, the use of AI in cancer care represents a brave new world, undoubtedly the wave of the future, but a world we must plan for carefully.
 Roberta Batorsky, MS, is a former university biology teacher and a freelance science journalist. She currently teaches Biology at a NJ state prison for youth.
Roberta Batorsky, MS, is a former university biology teacher and a freelance science journalist. She currently teaches Biology at a NJ state prison for youth.
The author would like to thank Dr. Rebecca Batorsky, Tufts University Institute for Artificial Intelligence (TIAI), for her assistance with this article.
This article was originally published in AWIS Magazine. Join AWIS to access the full issue of AWIS Magazine and more member benefits.