Scientists and clinicians now have an exciting new tool to help them detect and treat cancer: free-floating DNA fragments.
As we have known for decades, DNA consists of the genetic material stored inside the nucleus of cells in living organisms. Paul Mandel and Pierre Métais, French researchers who specialized in biological chemistry and medicine, first described free-floating DNA outside cells in human blood plasma in 1948. Nearly three decades later, scientists observed increased amounts of these fragments in the blood of cancer patients, corresponding with their disease stage and response to treatment. However, it took another 30–40 years—with improvements in DNA detection and amplification, development of next-generation sequencing in the 2000s, and advances in bioinformatics—to take advantage of these free-floating DNA fragments as accessible tools in managing cancer.
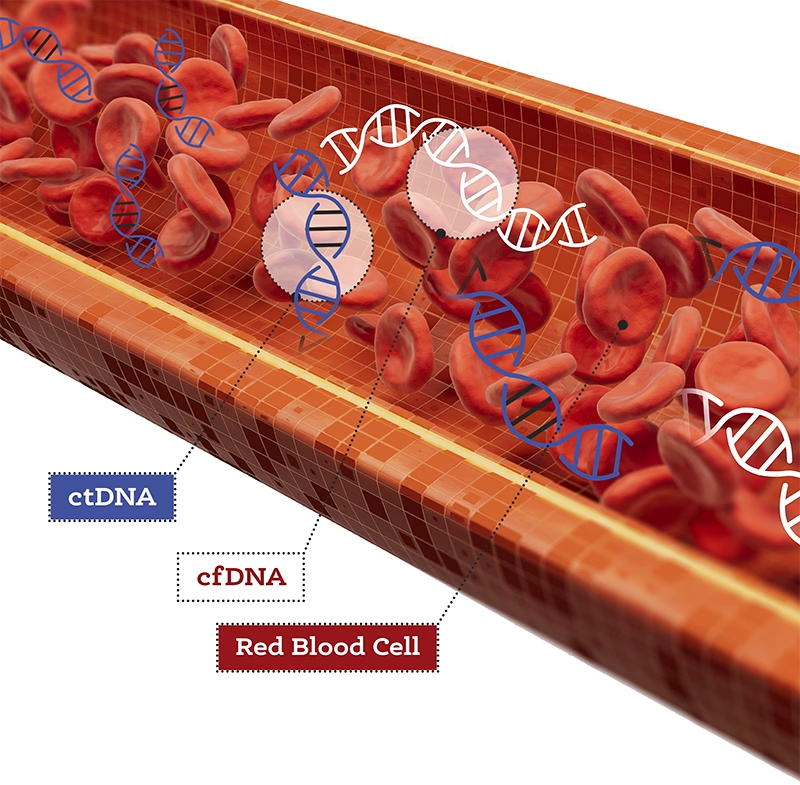
We now know that cells, including those from tumors, release DNA into the bloodstream and other bodily fluids as they die. Scientists refer to this substance as cell-free DNA (cfDNA). Circulating tumor DNA (ctDNA) is cfDNA released specifically by tumor cells. We can collect and analyze ctDNA to guide cancer diagnosis, molecular profiling, treatment selection, response to treatment, emergence of resistance mutations, detection of residual disease, and relapse.
Applications in Clinical Care
Oncologists can collect ctDNA through a blood draw, a less-invasive procedure than a tissue biopsy, which requires inserting a biopsy needle directly into the solid tumor. Another advantage of ctDNA is that it provides information from cells throughout the tumor, whereas a tissue biopsy collects samples from various sites in the tumor but may miss regions with genetically distinct subgroups of cancer cells. In the case of primary brain tumors, ctDNA levels are not as high in the bloodstream, likely due to the blood-brain barrier, but doctors can detect it in cerebrospinal fluid (CSF). They can collect CSF through a lumbar puncture and then analyze the ctDNA to detect mutations in the brain tumor and track genetic changes in it over time.
Currently, oncologists incorporate liquid biopsies in workups of patients with select cancer types. DNA sequencing, a technique that determines the nucleic acid sequence of a DNA molecule, allows them to identify genetic mutations in ctDNA. Doctors can use this information in turn to personalize cancer treatment selection by choosing the most effective therapies against a cancer with those mutations.
Importantly, liquid biopsies also provide quantification of ctDNA, or levels of ctDNA in the bloodstream. These levels (typically expressed as copies of mutant allele per milliliter) correlate with disease stage. For example, a patient with early-stage cancer may have 10 copies of ctDNA per 5 mL of plasma, whereas a patient with Stage IV cancer may have 100–1000 copies. Furthermore, oncologists can use these ctDNA levels to infer tumor size in response to treatment or relapse. A tumor that responds to treatment will shrink or disappear, and ctDNA levels decline, but if the tumor grows, ctDNA levels rise.
The short half-life of cfDNA and noninvasive blood draws make serial liquid biopsies feasible to monitor a patient’s response to treatment over time. By collecting liquid biopsies at different times—before, during, and after treatment—doctors can analyze ctDNA levels to infer changes in tumor size. In addition, they can evaluate ctDNA in the serial liquid biopsies to learn whether the tumor has acquired new mutations (referred to as clonal evolution), possibly as a form of drug resistance. Finally, they can also use serial liquid biopsies to detect relapse. If ctDNA levels rebound after treatment, it could be a sign that the cancer has returned.
Technological Advances Allow Adoption of ctDNA to Guide Treatment
Researchers initially faced two major hurdles that slowed their adoption of ctDNA analysis in the clinical care of cancer patients: how to identify mutations in small quantities of DNA material and how to distinguish between DNA that comes from tumor cells and DNA released by healthy cells. Fortunately, technological advances in high-throughput, next-generation sequencing, combined with increasingly sophisticated bioinformatics tools, now allow scientists and clinicians to unlock cancer information from minute quantities of free-floating DNA in the bloodstream.
 DNA sequencing has existed since 1977, when Frederick Sanger first developed it. What technological advances have allowed scientists to detect low levels of tumor DNA collected in a vial of blood? A key advance has been the increased sensitivity of molecular biology techniques for detection and sequencing of low levels of DNA. Being able to distinguish a true signal from background noise is critical.
DNA sequencing has existed since 1977, when Frederick Sanger first developed it. What technological advances have allowed scientists to detect low levels of tumor DNA collected in a vial of blood? A key advance has been the increased sensitivity of molecular biology techniques for detection and sequencing of low levels of DNA. Being able to distinguish a true signal from background noise is critical.
The technology that allows amplification (making more copies) of a DNA fragment—polymerase chain reaction (PCR)—has been around since 1983, and researchers often take this step before they sequence the DNA. Newer PCR technologies include digital PCR (dPCR) on microfluidic platforms, introduced in 1999, which enables accurate identification and quantification of low-abundance DNA fragments. However, dPCR is limited in the number of mutations it can test in a given sample. The development of high-throughput, next-generation sequencing technologies, which allow the sequencing of millions of DNA fragments in parallel, allows scientist to examine multiple genes for mutations.
Thus, next-generation sequencing allows oncologists to identify mutations and other genetic alterations across many genes in a given sample. Although analysis of next-generation sequencing data does not require a priori knowledge of gene mutations present in the tumor, having genetic results from a patient’s tissue biopsy can improve sensitivity of the sequencing assay and reduce background error rate. Thus, when possible, analysis of liquid biopsies goes hand in hand with analysis of tissue biopsies.
CtDNA is typically shorter than cfDNA released by normal cells (<100 base pairs [bp] versus around 167 bp) and has different fragmentation patterns. DNA fragment-length distribution helps oncologists distinguish ctDNA from normal cfDNA and offers them an additional layer of information when they interpret sequencing data for mutations found in the tumor. In addition to DNA sequence and fragment-length profiles, they can glean other information, such as epigenetic signatures, from ctDNA molecules. Epigenetic signatures are patterns of chemical modifications on DNA and the histone proteins which DNA wraps around. One type of epigenetic signature is DNA methylation, or the addition of methyl groups to DNA. Tumor tissues have different methylation profiles from normal tissue, so scientists can use it to distinguish ctDNA from cfDNA.
In addition, doctors can incorporate data from nucleosome occupancy patterns to improve the sensitivity of their ctDNA analysis. Within the nucleus, genomic DNA is initially compacted by wrapping around a core of histone proteins, analogous to beads on a string, which scientists refer to as nucleosomes. Changes in the positioning and spacing of nucleosomes along DNA, known as nucleosome occupancy pattern, reflect changes in gene expression, or whether or not a gene is turned on to make RNA and protein. Methylation and nucleosome occupancy patterns also differ depending on tissue or cell-type, so incorporating this data with other ctDNA analysis can help doctors determine the location of the cancer.
Researchers have also developed computational modeling approaches to estimate the proportion of ctDNA within the cfDNA sample (referred to as tumor fraction), as opposed to DNA coming from healthy cells. In cancer patients, ctDNA can range from 0.005 to 11.7% of cfDNA up to >80% of cfDNA in patients with advanced metastatic tumors. Doctors must understand tumor fraction to harness ctDNA as a tool in patient care. Knowing a patient’s tumor fraction can provide insights into disease stage, and tracking the tumor fraction over time through serial liquid biopsies can provide insights into disease progression and response to treatment.
Future Outlook
Clearly, ctDNA analysis can provide a window into the genetic alterations found in a tumor and into quantifying the disease burden. Free-floating DNA in our bloodstream provides richer and easier-access information than a tissue biopsy does. In addition, the ability to conduct serial sampling to monitor tumor size and clonal evolution through a noninvasive blood draw now revolutionizes oncology. Further improvements in the analytical sensitivity of molecular profiling tools to increase ctDNA mutation detection and to run multiple assays in parallel from the same blood sample could strengthen the use of liquid biopsies in the clinic. Fundamentally, we need to further understand how tumor cells release ctDNA and what factors affect its turnover in the bloodstream. This information could provide a more complete picture of how ctDNA levels change in patients and how they may differ from patient to patient.
Researchers are currently conducting clinical trials to investigate whether doctors can use ctDNA in the prognosis of a variety cancers. Can ctDNA analysis help predict the chances for recovery or recurrence? Could doctors determine whether the presence of ctDNA in the blood can help them detect cancer in presymptomatic individuals? They may be able to use the detection of ctDNA in otherwise healthy individuals to move beyond just screening for cancer through conventional clinical detection (imaging, blood-based cancer markers), with the hope that early diagnosis and intervention could improve outcomes and survival.
 Isabel Lam, PhD, is a Program Administrator at Dana-Farber Cancer Institute and the Harvard Cancer Consortium involved in training and career development of early-career investigators. She holds a PhD in Biomedical Sciences from Gerstner Sloan Kettering Graduate School of Biomedical Sciences and was a Postdoctoral Research Fellow at Brigham and Women’s Hospital and Harvard Medical School.
Isabel Lam, PhD, is a Program Administrator at Dana-Farber Cancer Institute and the Harvard Cancer Consortium involved in training and career development of early-career investigators. She holds a PhD in Biomedical Sciences from Gerstner Sloan Kettering Graduate School of Biomedical Sciences and was a Postdoctoral Research Fellow at Brigham and Women’s Hospital and Harvard Medical School.
This article was originally published in AWIS Magazine. Join AWIS to access the full issue of AWIS Magazine and more member benefits.