
Improving diverse representation in clinical trials and research has been a federal policy priority for decades. Yet a new report from the National Academies of Sciences, Engineering, and Medicine makes clear that as a nation, we still have a long way to go to make our clinical research enterprise more equitable. Although there has been progress with the representation of white women in clinical trials and research, it has largely stalled when it comes to the participation of racial and ethnic minority groups.
This underrepresentation results not only in serious costs to the populations underrepresented, but also to science and to the nation. Lack of representation may lead to lack of access to medical interventions for the populations not represented in trials, and it compounds health disparities in these populations. In addition, lack of representation of these populations in clinical research costs the nation hundreds of billions of dollars.
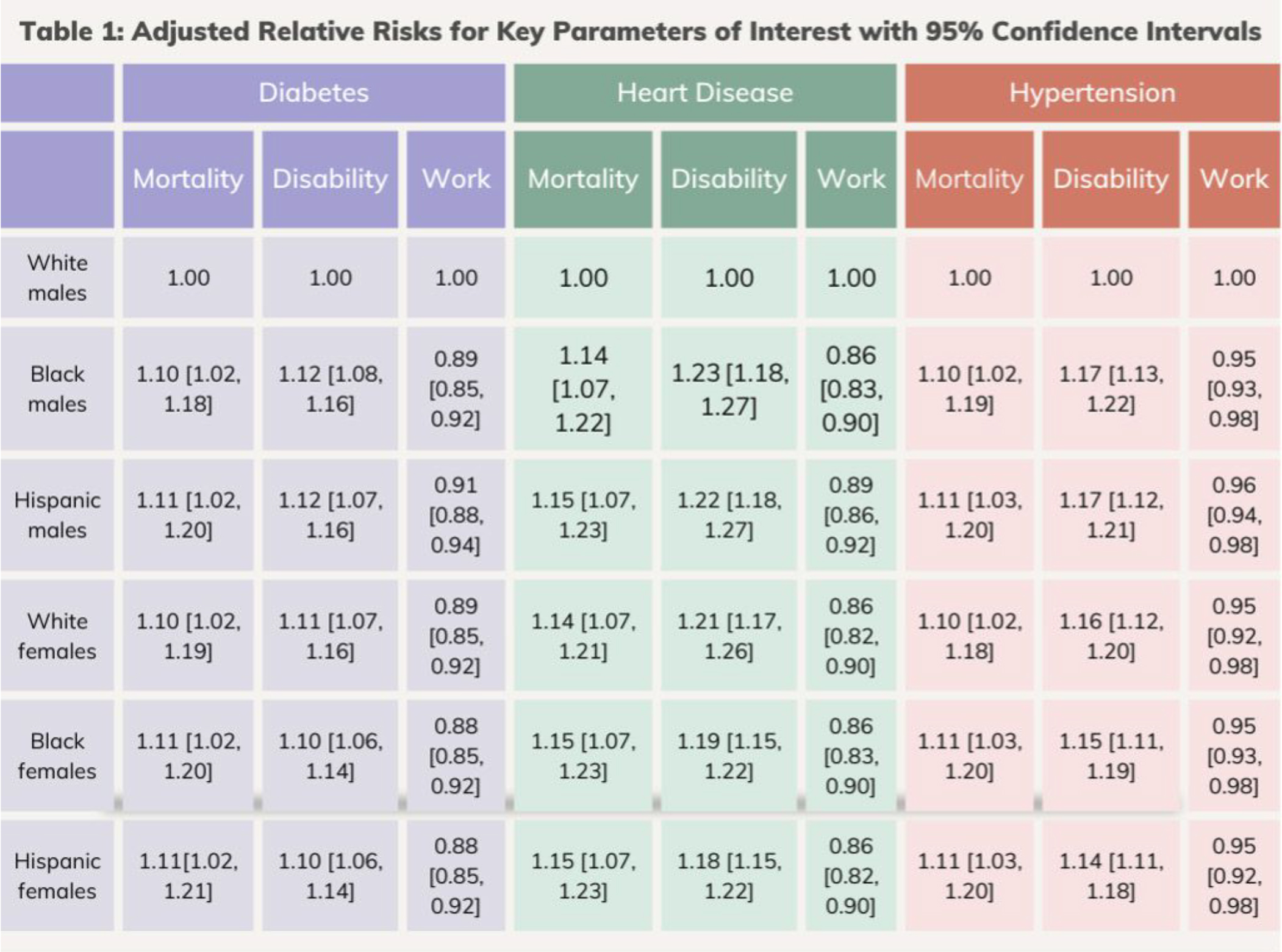
How exactly do we incur such costs? An economic analysis commissioned for the National Academies report demonstrated high financial and social costs to the lack of representation in clinical research, measured in lost lives, increased disability, and lost productivity. The economic analysis used the Future Elderly Model to estimate the social costs of health disparities for groups that have been historically underrepresented in clinical research. Non-Hispanic white men served as the reference group, due to their historical inclusion and representation in clinical trials and clinical research. The evidence shows that self-reported, nonHispanic Black men, Hispanic/Latinx men, non-Hispanic white women, non-Hispanic Black women, and Hispanic/ Latinx women all would potentially benefit from narrowing the differential impact of disease on the outcomes of mortality, disability, and loss of work (see Table 1).
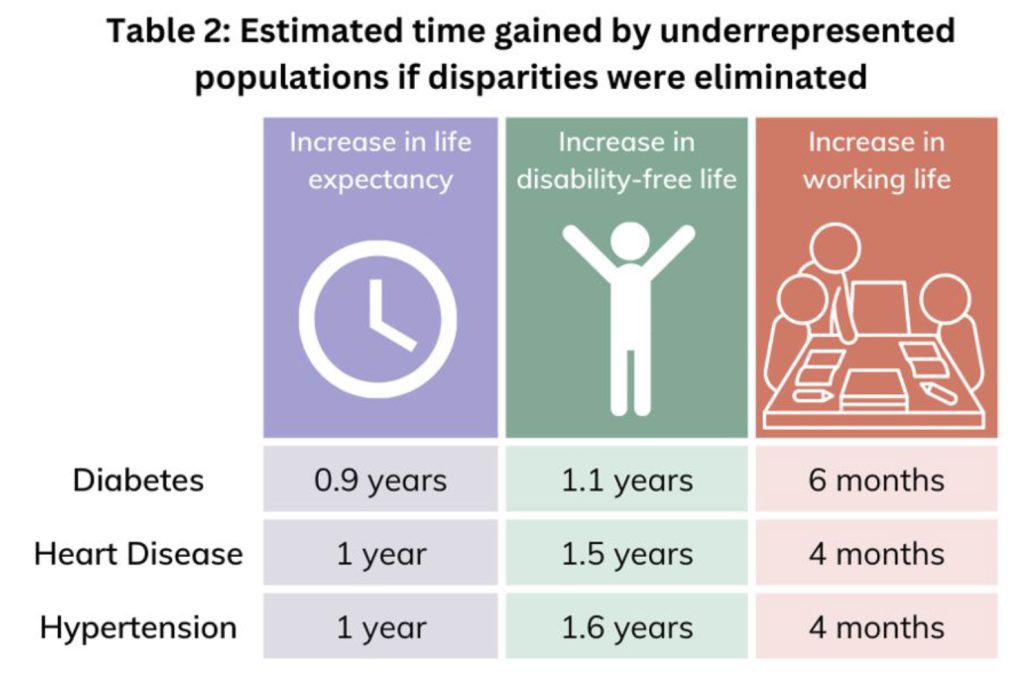 The committee charged with producing the report then considered potential benefits of reducing disparities for three key chronic diseases: diabetes, heart disease, and hypertension. The additional life expectancy, disability-free life expectancy, and working years in underrepresented population groups compared with what non-Hispanic White men experience for all three conditions can be found in Table 2. In aggregate, the committee found that if we continue on our current path, health disparities in diabetes will cost society more than $5 trillion through 2050— including in mortality, morbidity, and loss of work. Heart disease will cost more than $6 trillion, and hypertension even more.
The committee charged with producing the report then considered potential benefits of reducing disparities for three key chronic diseases: diabetes, heart disease, and hypertension. The additional life expectancy, disability-free life expectancy, and working years in underrepresented population groups compared with what non-Hispanic White men experience for all three conditions can be found in Table 2. In aggregate, the committee found that if we continue on our current path, health disparities in diabetes will cost society more than $5 trillion through 2050— including in mortality, morbidity, and loss of work. Heart disease will cost more than $6 trillion, and hypertension even more.
Therefore, health disparities incur a substantial toll on our nation. The committee acknowledges that better representation in clinical research is not all that is needed to reduce these disparities. However, if better representation reduced health disparities by only one percent through improved health access, increased discovery and innovation, and increased trust, it would result in more than $40 billion in gains for diabetes and $60 billion for heart disease alone.
This research makes a compelling case for why urgent and immediate action is needed to create better representation in our nation’s clinical trials and clinical research.
 Alex Helman, PhD is a senior program officer at the National Academies of Sciences, Engineering, and Medicine and was the study director for the featured report, Improving Representation in Clinical Trials and Research: Building Research Equity for Women and Underrepresented Groups. During her time at the Academies, Dr. Helman has directed multiple consensus studies focused on improving research equity and was the lead of the Prevention Working Group and the Evaluation Working Group for the Action Collaborative on Preventing Sexual Harassment in Higher Education. Currently, Dr. Helman is leading a new consensus study focused on the state of liability around research conducted in pregnant and lactating persons. Before joining the National Academies full time, Dr. Helman was a 2018 Christine Mirzayan Science and Technology Policy Graduate Fellow at the National Academies. Dr. Helman received her PhD in molecular and cellular biochemistry from the University of Kentucky and her BS in biochemistry from Elon University.
Alex Helman, PhD is a senior program officer at the National Academies of Sciences, Engineering, and Medicine and was the study director for the featured report, Improving Representation in Clinical Trials and Research: Building Research Equity for Women and Underrepresented Groups. During her time at the Academies, Dr. Helman has directed multiple consensus studies focused on improving research equity and was the lead of the Prevention Working Group and the Evaluation Working Group for the Action Collaborative on Preventing Sexual Harassment in Higher Education. Currently, Dr. Helman is leading a new consensus study focused on the state of liability around research conducted in pregnant and lactating persons. Before joining the National Academies full time, Dr. Helman was a 2018 Christine Mirzayan Science and Technology Policy Graduate Fellow at the National Academies. Dr. Helman received her PhD in molecular and cellular biochemistry from the University of Kentucky and her BS in biochemistry from Elon University.